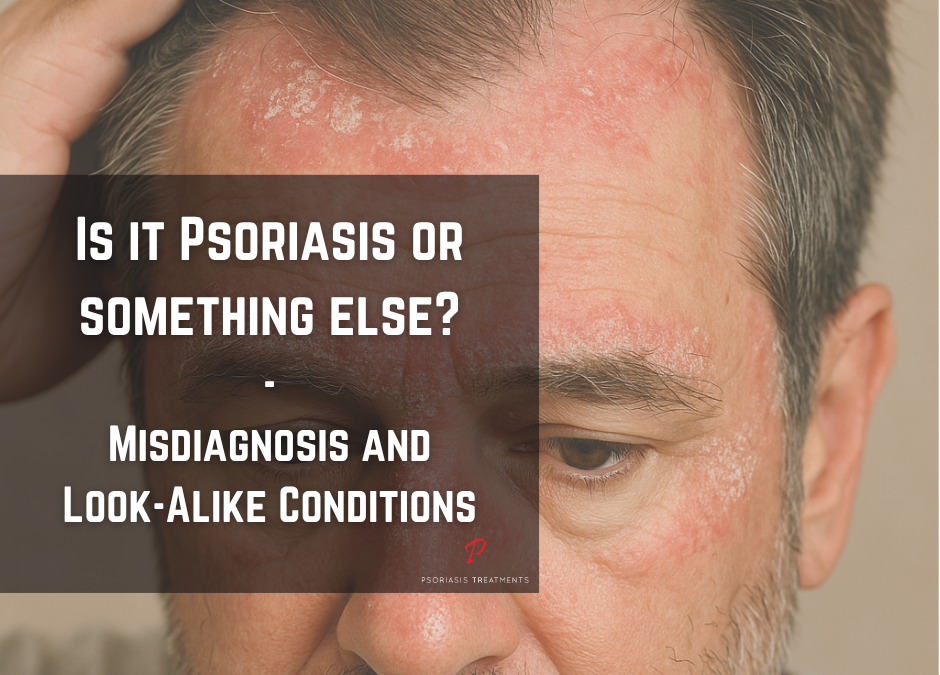
Psoriasis misdiagnosis is common because several inflammatory and infectious skin diseases can appear very similar during early stages. Redness, scaling, and itching often occur across multiple dermatologic conditions. Because of this overlap, early psoriasis may be confused with eczema, fungal infections, or dermatitis before full symptom patterns develop.
Recognizing how psoriasis is commonly misdiagnosed helps patients seek earlier evaluation and receive more appropriate treatment. In addition, understanding key differences between similar skin conditions can reduce delays in diagnosis and support better long term disease management.
Psoriasis Misdiagnosis: Why It Happens and Why It Is Common
Psoriasis misdiagnosis often occurs because early symptoms overlap with other skin disorders. For example, redness, dry patches, and itching can appear in both inflammatory and infectious skin diseases. However, psoriasis typically produces thicker plaques and more defined scaling patterns, which usually become clearer as the disease progresses.
Symptom location can also vary significantly. While psoriasis often affects elbows, knees, and the scalp, other conditions may appear in skin folds or moisture-prone areas. Because of this variation, diagnosis based only on visual appearance can sometimes be misleading.
If you are unsure whether your symptoms match psoriasis, reviewing a full medical overview of psoriasis causes, symptoms, and treatment options can help clarify typical patterns and disease progression.
How Doctors Reduce Psoriasis Misdiagnosis Risk
Dermatologists usually combine physical examination with patient history and symptom timing to improve diagnostic accuracy. In many cases, they also review family history and previous flare patterns to identify chronic inflammatory disease patterns. Furthermore, when symptoms remain unclear, doctors may recommend skin biopsy or laboratory testing to confirm diagnosis and rule out infection or other inflammatory skin diseases.
Clinical guidance from major dermatology organizations, including resources from the American Academy of Dermatology, emphasizes that early and accurate diagnosis improves treatment success and helps reduce long term inflammation risk.
Psoriasis Misdiagnosis and Skin Conditions Commonly Confused With Psoriasis
Several diseases may be mistaken for psoriasis, particularly when symptoms are mild or appear in unusual locations. Because of this overlap, understanding psoriasis misdiagnosis helps prevent incorrect treatment approaches and supports earlier, more accurate diagnosis.
Eczema vs Psoriasis

Eczema often appears as red, itchy patches in body creases such as elbows, knees, and neck folds.
In eczema, skin changes usually appear as red, itchy patches in body creases such as elbows, knees, and neck folds. These areas may also become very itchy, especially during flare periods. In contrast, psoriasis plaques usually have thicker scaling and clearer borders. In addition, eczema symptoms may fluctuate quickly, while psoriasis plaques typically persist longer and follow a chronic inflammatory pattern. If you want to learn more, you can review detailed comparisons explaining key differences between psoriasis and eczema and how to recognize them early.
Seborrheic dermatitis vs. Psoriasis

This scalp condition can mimic scalp psoriasis.
Seborrheic dermatitis, which causes flaking and irritation on the scalp, face, or upper chest, can resemble scalp psoriasis. However, psoriasis usually produces thicker, more defined plaques with dry scaling. In contrast, seborrheic dermatitis tends to produce yellowish flakes and greasy redness.
Fungal Infection vs Psoriasis

Ringworm presents as an itchy, ring-like rash and can be mistaken for psoriasis or eczema.
Fungal infections may produce red or scaly patches, especially in warm or moist skin areas. However, fungal infections often create ring-shaped lesions or clearer borders, while psoriasis typically forms thicker plaques with silvery scale. Because of this similarity, psoriasis misdiagnosis sometimes occurs when antifungal treatment is used first without improvement.
Dermatitis vs Psoriasis
Dermatitis may cause redness and irritation triggered by allergens or irritants. However, dermatitis usually improves quickly with topical treatment. In contrast, psoriasis usually requires long term inflammation control and monitoring.
Additional Conditions That May Be Mistaken for Psoriasis
Some less common inflammatory or autoimmune diseases can also resemble psoriasis, especially when symptoms appear in unusual locations or follow atypical patterns. In these cases, dermatologists may use additional diagnostic testing or longer monitoring to confirm the correct diagnosis.
Pityriasis rosea vs Psoriasis

It often starts with a herald patch and then spreads in a “Christmas tree” pattern across the trunk.
Pityriasis rosea is a temporary skin condition that can mimic psoriasis, especially guttate psoriasis. It often starts with a single large herald patch on the trunk, followed by smaller scaly spots that follow skin tension lines. Unlike psoriasis, pityriasis rosea typically resolves on its own within a few months.
Lupus vs Psoriasis
In some cases, lupus-related skin conditions such as discoid lupus can produce red, scaly plaques that resemble psoriasis. However, lupus rashes may scar or leave pigment changes, and they often worsen with sun exposure. In addition, systemic lupus can cause fatigue or fever, which are not typical symptoms of psoriasis.
How Joint and Systemic Symptoms Help Confirm Diagnosis

Rheumatoid arthritis causes symmetrical joint swelling and stiffness, often confused with psoriatic arthritis.
Joint and systemic symptoms can help differentiate psoriasis-related conditions from other diseases. For example, psoriatic arthritis can be confused with other types of arthritis, especially rheumatoid arthritis. However, psoriatic arthritis often causes swelling in the fingers or toes, sometimes affecting the entire digit. In contrast, it usually affects joints asymmetrically and can also cause pain at tendon attachment points, while rheumatoid arthritis typically affects the same joints on both sides of the body.
Why Accurate Diagnosis Matters
Several inflammatory and infectious skin diseases can resemble psoriasis during early stages. Many patients experience redness, scaling, and itching across multiple dermatologic conditions. As a result, early psoriasis may be confused with eczema, fungal infections, or dermatitis before full symptom patterns develop.
Practical Ways to Get to the Right Diagnosis
Specialists such as dermatologists and rheumatologists are best equipped to evaluate these complex cases. In addition, diagnostic tools like skin biopsy, blood tests, or even a symptom diary can provide valuable clinical clues. Photos of previous flare-ups can also help show how symptoms have changed over time.

Nail fungus causes thick, discolored nails and may resemble psoriatic nail changes.
Even if you have been treated for a specific diagnosis for years, it may be worth reassessing if symptoms change or stop responding to treatment. Because psoriasis and similar conditions are well studied, clinicians usually have reliable methods to distinguish between them. In some cases, seeking a second opinion can significantly improve diagnostic accuracy.
Understanding psoriasis misdiagnosis and similar skin conditions helps prevent delayed treatment and incorrect therapy choices. As a result, earlier evaluation and correct diagnosis can significantly improve long term disease outcomes.
Long Term Management After Correct Diagnosis
Delayed or incorrect diagnosis can allow inflammation to continue unchecked in chronic skin disease. Without treatment, symptoms may worsen or spread before correct therapy is started. In addition, untreated psoriasis may increase the risk of systemic inflammatory complications affecting joints and metabolic health.
Once the correct diagnosis is confirmed, treatment plans can be adjusted to match disease severity, symptom location, and overall health factors. In many cases, long term management may include topical therapy, phototherapy, or systemic immune-targeted treatments. Furthermore, monitoring symptoms over time helps doctors adjust treatment and reduce flare frequency.
Conditions That Are Most Frequently Mistaken for Psoriasis in Clinical Practice
| Condition | Why It’s Similar | Key Differences |
|---|---|---|
| Eczema (Atopic Dermatitis) | Red, itchy patches; can scale | Eczema is itchier, usually starts in childhood, favors creases (e.g. inside elbows), and may ooze. Psoriasis tends to be thicker, with silvery scale and on outer elbows/knees. |
| Seborrheic Dermatitis (Dandruff) | Flaky scalp, redness | Dandruff is greasy/yellowish with oily scalp; psoriasis is dry, thick, and silvery. Psoriasis often extends beyond the hairline. |
| Fungal Infections (e.g. Ringworm, Jock Itch) | Red, scaly patches | Fungal rashes are ring-shaped with clear centers. Psoriasis plaques are more uniform and not circular. Fungal infections often itch more intensely. |
| Pityriasis Rosea | Red, scaly rash | Starts with a single “herald patch” and resolves on its own in 6–8 weeks. Psoriasis is chronic and lacks this pattern. Often affects teens/young adults. |
| Lupus (Cutaneous or Systemic) | Red scaly plaques, joint pain | Lupus often leaves scars, is sun-sensitive, and may cause systemic symptoms (fever, fatigue). Psoriasis is more localized to skin/joints and rarely causes systemic illness. |
| Rheumatoid Arthritis (RA) | Joint pain and swelling | RA is symmetric and hits different joints than psoriatic arthritis. PsA may also cause skin plaques and “sausage” digits (dactylitis). |
| Osteoarthritis (OA) | Joint pain and stiffness | OA is degenerative (wear-and-tear), not autoimmune. PsA affects younger people, often with morning stiffness and nail changes. |
| Gout | Sudden joint swelling and pain | Gout comes in acute attacks, often in the big toe. PsA is more chronic and widespread. |
| Nail Fungus | Thick, discolored nails | Fungal nails can mimic nail psoriasis. A lab test can distinguish them. |
| Lichen Planus | Scaly, itchy patches | Typically purple-toned and flat-topped; often in wrists, ankles, and mouth. Psoriasis is usually red with silver scale. |
| Secondary Syphilis | Widespread scaly rash | May affect palms/soles; rare but can look like guttate psoriasis. Confirmed via blood tests. |
| Skin Cancer | Scaly or bleeding lesions | Unusual or changing patches could be cancer (e.g. squamous cell carcinoma). Biopsy is needed if a plaque doesn’t behave like usual psoriasis. |
The Importance of Correct Diagnosis in Chronic Skin Disease
Accurate diagnosis is essential for effective long term treatment planning. When skin symptoms are persistent, unusual, or resistant to standard therapy, medical evaluation helps distinguish psoriasis from other inflammatory or infectious skin diseases. As a result, earlier recognition reduces treatment delays and improves long term inflammatory disease control.